Dear Middle-Aged Woman: A Peep into Osteoarthritis in 2024
Peace Aláwodé
Dear middle-aged woman. The body is funny, isn’t it?
Yours, like many, might have started feeling like its best-before date is near. You might have started appreciating some realities better. Like, how well you enjoy your body, depends on what you put in it and how you use it. But, do not be alarmed.
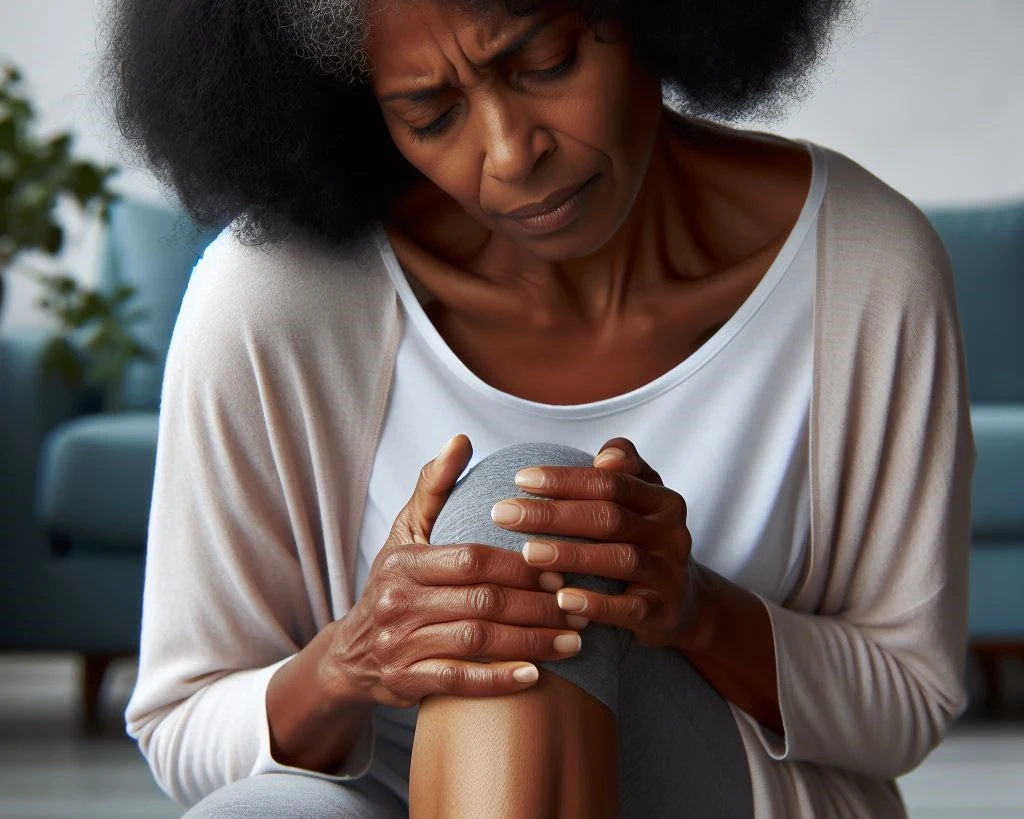
Now let’s talk about a few things. You see, that pain you feel in your knees, particularly worse in the mornings and accompanied by some stiffness; comes with cracking sounds and gets a bit better after a few movements, has a name. It is Arthritis, and most commonly, Osteoarthritis.
Osteoarthritis (OA) is usually the cause of those symptoms. It is good to know that it not only affects the knee but also the hand, hip, and spine. And yes, one individual can have it all
Here, we will only talk about the knee and how to reduce your pain and reclaim your knee functions.
A look at statistics shows the following, that:
OA is the most common disease of the joints worldwide and the knee is the most commonly affected.
More than 80% of adults older than 55 have osteoarthritis, even if some of them never experience symptoms
Women are more commonly affected than men.
Also, it is seen to be prevalent among those of African descent.
Overweight women have nearly 4 times the risk of knee OA; for overweight men, the risk is 5 times greater. Meaning that women of African ancestry and are overweight have a high chance of this.
So, by definition, OA is a condition that causes joints to become painful and stiff, and the cartilage to wear away. It is a degenerative disease with an inflammatory component. It affects the cartilage, bone, and synovial fluid (lubricant) of your joint. The following are usually the complaints and yours might fall into one or a few of them:
Knee pain that is gradual in onset and worsens with activity
Stiffness, particularly early morning stiffness (lasting less than 30 minutes)
Loss of range of movement and knee functions
Pain after prolonged sitting or resting
Pain on handling/touching the joint
Joint enlargement and swelling
Crepitus or a cracking sound with joint movement
The direct causes of OA aren’t yet clearly established, but can be roughly grouped into:
Primary OA which are thought to be due to age and are of unknown origin
Secondary OA which are due to known causes e.g. joint injury and obesity.
Though anyone can develop OA, adults older than 55 years, adults who are Menopausal, and those with obesity, diabetes, high cholesterol levels, and autoimmune diseases are highly at risk.
The progression of osteoarthritis is normally slow, occurring over several years or decades. Over this period, there’s the risk of becoming less and less active which can open the door to other health challenges like weight gain, and obesity.
Initially, the pain can be relieved by rest and may respond to simple pain medications. However, your joints may become unstable as the osteoarthritis progresses; therefore, the pain may become more prominent (even during rest) and may not respond to medications.
Hence, we come to the rehabilitative care for the knee. Knee OA is best managed initially by non-surgical means, after which if these fail, then, is surgery recommended.
The first step is being educated about the condition and how it can best be managed. This is best done by a healthcare specialist. Also, it can be beneficial to read from trusted sources.
The use of analgesics like acetaminophen (Tylenol) and NSAIDs (Ibuprofen, Diclofenac) is proven to be beneficial in pain reduction. This can be topical or oral.
Exercise therapy and prescription
Activity modification
Advice on weight loss
Use of knee bracing,
Use of heat and Ice
Self-management
The list above is within the scope and practice of Orthopedic Physiotherapists and they are the best clinicians to help you through your recovery. You can reach out to your healthcare provider or contact us to schedule an online consultation with a licensed Orthopedic Physiotherapist.
The role of the Physiotherapist includes educating you and promoting your skills of self-management. This has been shown to aid in better health outcomes.
Exercise is at the core of OA conservative treatment. Research shows that combining exercise with a good diet leads to pain relief, improvement in mobility, significant reduction in weight and total fat mass,
Excessive fat tissue, as it occurs in obesity, increases stresses on weight-bearing joints and eventually lead to cartilage breakdown as seen in OA.
Low-contact sports (like walking, cycling, elliptical cycling), mind and body exercises such as Tai Chi and yoga, and aquatic exercises (like swimming) to name a few have been seen to be very beneficial. They prevent maximum joint stress and improve muscle strength and joint stability. High-contact sports preferably should be avoided.
Conclusion
You need to know that knee OA has no cure, but interventions and management can be targeted toward slowing its progression and reducing symptoms. The goal is to minimize knee pain, optimize function, and support self-management.
There are conservative and operative means. Usually, upon diagnosis, conservative methods are first considered before surgery. Self-management falls under the conservative pathway and has been shown to give great results when done along with specialist Physiotherapy care and advice.
Like this project
Posted Jul 7, 2024
Dear middle-aged woman, that pain you feel in your knees, particularly worse in the mornings and accompanied by some stiffness, comes with cracking sounds and…
Likes
0
Views
6